

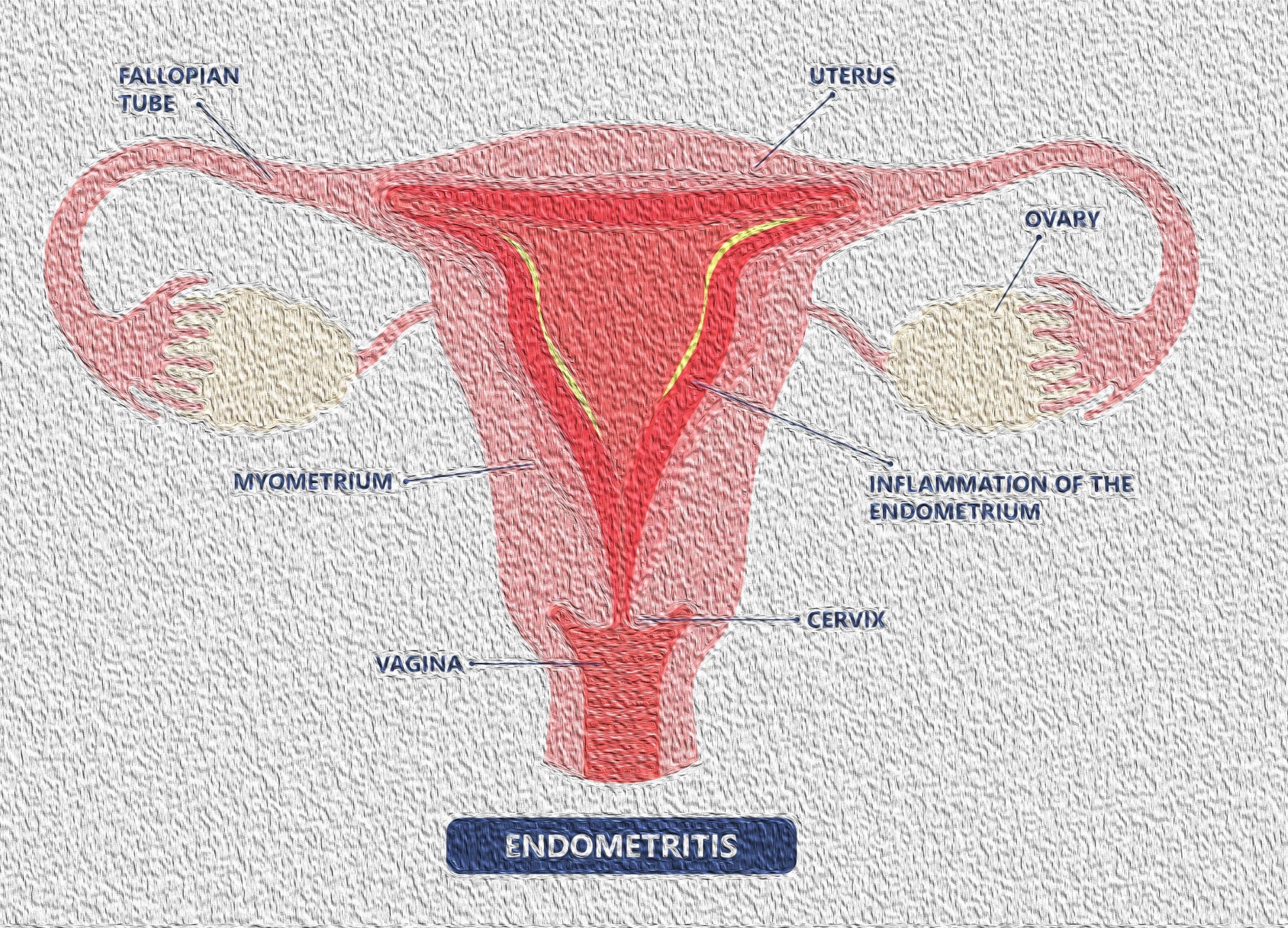
Endometritis is also often associated with inflammation of the fallopian tubes (salpingitis), ovaries (oophoritis), and pelvic peritoneum (pelvic peritonitis. From a pathologic perspective, endometritis can be classified as acute versus chronic.
The diagnosis of acute endometritis is based on clinical findings, such as fever and lower abdominal pain, however, chronic endometritis is most commonly an asymptomatic condition without manifestation.
Infection of the endometrium usually results from an ascending infection from the lower genital tract. In the general population, chronic endometritis has been seen with infections (e.g., chlamydia, tuberculosis, bacterial vaginosis) and the presence of an intrauterine device.
Endometritis is a polymicrobial disease involving, on average, 2-3 organisms. In most cases, it arises from an ascending infection from organisms found in the normal indigenous vaginal flora.
Commonly isolated organisms include Ureaplasma urealyticum, Peptostreptococcus, Gardnerella vaginalis, Bacteroides bivius, and group B Streptococcus. Chlamydia has been associated with late-onset postpartum endometritis. Enterococcus is identified in up to 25% of women who have received cephalosporin prophylaxis. Herpes and tuberculosis are rare causes, although in some countries tuberculosis is not an uncommon etiologic agent.
For acute endometritis diagnosis usually is based on clinical findings, like:
- Fever
- Lower abdominal pain
- Foul-smelling lochia in the obstetric population
- Abnormal vaginal bleeding
- Abnormal vaginal discharge
- Dyspareunia (pain during intercourse)
- Dysuria (pain when urinating)
- Malaise
However, chronic endometritis tends to be indolent, with no significant constitutional symptoms.
The following factors increase the risk for endometritis in general:
- Presence of an intrauterine device: the vaginal part of the device may serve as a track for the organisms to ascend into the uterus
- Presence of menstrual fluid in the uterus
- Associated cervicitis secondary to gonorrhea or Chlamydiainfection
- Associated bacterial vaginosis
- Frequent douching
- Unprotected sexual activity
- Multiple sexual partners
- Use of swimming pools, public toilets
- Cervical ectopy
Fertility Complications
Chronic endometritis changes the naturally receptive for embryos endometrium into a toxic and hostile environment. Survival and implantation of the embryos is inhibited thus, causing infertility, recurrent IVF failures or even early miscarriages. Spread of infection from the endometrium to the fallopian tubes, ovaries, or the peritoneal cavity may result in salpingitis, oophoritis, localized peritonitis, or tubo-ovarian abscesses. Salpingitis subsequently leads to tubal dysmotility and adhesions that result in infertility, higher incidence of ectopic pregnancy, and chronic pelvic pain.
Chronic endometritis is thus associated with infertility and recurrent IVF failures and early pregnancy loss. It is a subtle condition and is therefore difficult to diagnose.
Endometrial tissue biopsy or alternatively menstrual blood can be obtained to assess chronic endometritis in the general population.
Treatment
Antibiotic therapy with usually a combination of drugs is indicated.
Clindamycin and gentamicin have been considered the criterion standard treatment. The combination of a second- or third-generation cephalosporin with metronidazole is another potential choice. In cases that an analytical report of the uterine bacterial flora, obtained by endometrial sampling is available, antibiotic treatment is targeted towards the specific microorganisms detected.

